Prescribing and Administration Monographs
General Information
Clinical Guidelines and Protocols
Antimicrobial Guidelines
Disclaimer
Hyperkalaemia: See also CHI Acute Management of Hyperkalaemia Guideline
intravenous: 4microgram/kg IV bolus
Nebuliser: 1.25mg-2.5mg via nebuliser, repeat if required. IV route preferred.
Acute asthma: See also Asthma Guidelines: Acute Asthma (ED care) , Acute Asthma (Inpatient) and Asthma: Management of Severe and Life-threatening Disease
For infants < 1year old, discuss treatment with Senior Medical Registrar.
Mild and moderate bronchoconstriction (i.e. asthma)
< 6 years: 600 microgram (6 puffs: equivalent to one dose) inhaled every 20 minutes for 1 hour. Review 20 minutes after 3rd dose.
≥6 years: 1200 microgram (12 puffs: equivalent to one dose) inhaled every 20 minutes for 1 hour. Review 10 – 20 minutes after 3rd dose to decide on admission or discharge.
Severe bronchoconstriction (i.e. asthma):
6months - < 5years: 2.5mg via nebuliser
≥5 years: 5mg via nebuliser
OR the following weight based dosing can be used: 0.15mg/kg (maximum 5mg)
Give above doses every 20 minutes for 1 hour. Review on-going requirements 10-20 minutes after 3rd dose.
Critical bronchoconstriction (i.e. asthma):
Where nebulisation has failed, a continuous intravenous infusion should be commenced at a rate of 1–2 microgram/kg/minute. Adjust if required to a maximum rate of 5 micrograms/kg/minute, according to response and heart rate. Higher doses have been used. Administer in PICU setting with cardiac monitoring.
Note: Usual adult dose range 3-20microgram/minute. These doses will be exceeded quickly in larger children; monitor closely. See Monitoring and Adverse Effects sections.
Chronic therapy, prophylaxis of exercise or allergen induced bronchospasm:
100 – 200microgram (one to two puffs) inhaled up to 4 times daily
Severe hyperkalaemia: See also CHI Acute Management of Hyperkalaemia Guideline
Intravenous: 4microgram/kg, may be repeated if necessary.
Nebulised: 2.5 - 5mg, repeated if necessary. IV route preferred.
Cardiac / ECG monitoring: for patients receiving a continuous intravenous infusion.
Lactic acidosis: Increase in lactate levels (in association with high therapeutic doses of salbutamol) may lead to dyspnoea and compensatory hyperventilation, which could be misinterpreted as a sign of asthma treatment failure and lead to inappropriate intensification of salbutamol therapy. Monitor closely for the developement of elevated serum lactate and consequent metabolic acidosis in this setting.
Salbutamol toxicity and genuine clinical deterioration are easily confused, and reducing or stopping the infusion may need to be trialled.
Hypokalaemia: monitor potassium levels (increased risk of arrhythmias)
Hyperglycaemia: monitor blood glucose and lactate levels, especially in diabetic patients.
Inhaled: Using Ventolin Evohaler Metered Dose Inhaler (100 microgram salbutamol per actuation)
A suitable spacer device (Babyhaler / Aerochamber / Volumatic) available from Pharmacy should be used to facilitate administration in smaller children.
Nebulised: Using Ventolin Nebules 2.5mg or 5mg
Administer undiluted via a suitable nebuliser. If deliver time > 10 minutes is required, can dilute with sterile Sodium Chloride 0.9%w/v.
Intravenous: Use Ventolin® Concentrate for infusion 1mg/mL
Compatible infusion fluids: Sodium Chloride 0.9%w/v or Glucose 5%w/v.
Method of administration:
Asthma: Administer by continuous intravenous infusion via the CHI Smart-pump Standard Concentration Infusion (SCI) drug library.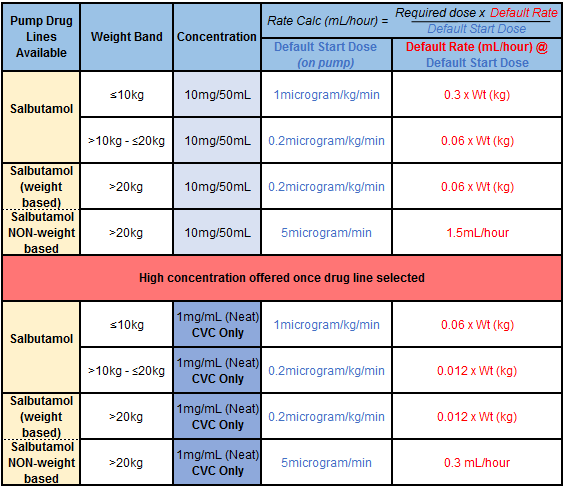
Hyperkalaemia:
Slow IV bolus over 5 minutes: Dilute required dose to a concentration of 50 microgram/mL (please note different concentration to the continuous infusion)
To prepare a 10mL solution of 50 micrograms/mL:
• Dilute salbutamol 500 micrograms (0.5mL of 1mg/mL neat preparation) with 9.5mLs of diluent. Mix well.
• Draw up the volume required and administer by slow intravenous injection over 5 minutes
Non-selective beta-adrenoreceptors e.g. propranolol; salbutamol can inhibit their effect.
Potassium depleting agents e.g. diuretics, corticosteroids, digoxin; increased risk of hypokalaemia.
For all beta-2-adrenoreceptor agonists: Arrhythmias; dizziness; headache; hypokalaemia (with high doses); nausea; palpitations; tremor; hyperglycaemia; bronchospasm (rare).
For salbutamol: Muscle cramps; vasodilation; metabolic changes
Beware of signs of potential toxicity (both IV and inhaled therapy): tachycardia; tachypnoea; metabolic acidosis (lactate commonly high); hypokalaemia
This list is not exhaustive, see SPC www.hpra.ie for full details.
Ventolin® Evohaler 100microgram/puff
Salamol® Steri-neb 2.5mg/2.5mL
Ventolin® Concentrate for Infusion 1mg/mL
Hyperkalaemia: See also CHI Acute Management of Hyperkalaemia Guideline
intravenous: 4microgram/kg IV bolus
Nebuliser: 1.25mg-2.5mg via nebuliser, repeat if required. IV route preferred.
Acute asthma: See also Asthma Guidelines: Acute Asthma (ED care) , Acute Asthma (Inpatient) and Asthma: Management of Severe and Life-threatening Disease
For infants < 1year old, discuss treatment with Senior Medical Registrar.
Mild and moderate bronchoconstriction (i.e. asthma)
< 6 years: 600 microgram (6 puffs: equivalent to one dose) inhaled every 20 minutes for 1 hour. Review 20 minutes after 3rd dose.
≥6 years: 1200 microgram (12 puffs: equivalent to one dose) inhaled every 20 minutes for 1 hour. Review 10 – 20 minutes after 3rd dose to decide on admission or discharge.
Severe bronchoconstriction (i.e. asthma):
6months - < 5years: 2.5mg via nebuliser
≥5 years: 5mg via nebuliser
OR the following weight based dosing can be used: 0.15mg/kg (maximum 5mg)
Give above doses every 20 minutes for 1 hour. Review on-going requirements 10-20 minutes after 3rd dose.
Critical bronchoconstriction (i.e. asthma):
Where nebulisation has failed, a continuous intravenous infusion should be commenced at a rate of 1–2 microgram/kg/minute. Adjust if required to a maximum rate of 5 micrograms/kg/minute, according to response and heart rate. Higher doses have been used. Administer in PICU setting with cardiac monitoring.
Note: Usual adult dose range 3-20microgram/minute. These doses will be exceeded quickly in larger children; monitor closely. See Monitoring and Adverse Effects sections.
Chronic therapy, prophylaxis of exercise or allergen induced bronchospasm:
100 – 200microgram (one to two puffs) inhaled up to 4 times daily
Severe hyperkalaemia: See also CHI Acute Management of Hyperkalaemia Guideline
Intravenous: 4microgram/kg, may be repeated if necessary.
Nebulised: 2.5 - 5mg, repeated if necessary. IV route preferred.
Cardiac / ECG monitoring: for patients receiving a continuous intravenous infusion.
Lactic acidosis: Increase in lactate levels (in association with high therapeutic doses of salbutamol) may lead to dyspnoea and compensatory hyperventilation, which could be misinterpreted as a sign of asthma treatment failure and lead to inappropriate intensification of salbutamol therapy. Monitor closely for the developement of elevated serum lactate and consequent metabolic acidosis in this setting.
Salbutamol toxicity and genuine clinical deterioration are easily confused, and reducing or stopping the infusion may need to be trialled.
Hypokalaemia: monitor potassium levels (increased risk of arrhythmias)
Hyperglycaemia: monitor blood glucose and lactate levels, especially in diabetic patients.
Inhaled: Using Ventolin Evohaler Metered Dose Inhaler (100 microgram salbutamol per actuation)
A suitable spacer device (Babyhaler / Aerochamber / Volumatic) available from Pharmacy should be used to facilitate administration in smaller children.
Nebulised: Using Ventolin Nebules 2.5mg or 5mg
Administer undiluted via a suitable nebuliser. If deliver time > 10 minutes is required, can dilute with sterile Sodium Chloride 0.9%w/v.
Intravenous: Use Ventolin® Concentrate for infusion 1mg/mL
Compatible infusion fluids: Sodium Chloride 0.9%w/v or Glucose 5%w/v.
Method of administration:
Asthma: Administer by continuous intravenous infusion via the CHI Smart-pump Standard Concentration Infusion (SCI) drug library.
Hyperkalaemia:
Slow IV bolus over 5 minutes: Dilute required dose to a concentration of 50 microgram/mL (please note different concentration to the continuous infusion)
To prepare a 10mL solution of 50 micrograms/mL:
• Dilute salbutamol 500 micrograms (0.5mL of 1mg/mL neat preparation) with 9.5mLs of diluent. Mix well.
• Draw up the volume required and administer by slow intravenous injection over 5 minutes
Non-selective beta-adrenoreceptors e.g. propranolol; salbutamol can inhibit their effect.
Potassium depleting agents e.g. diuretics, corticosteroids, digoxin; increased risk of hypokalaemia.
For all beta-2-adrenoreceptor agonists: Arrhythmias; dizziness; headache; hypokalaemia (with high doses); nausea; palpitations; tremor; hyperglycaemia; bronchospasm (rare).
For salbutamol: Muscle cramps; vasodilation; metabolic changes
Beware of signs of potential toxicity (both IV and inhaled therapy): tachycardia; tachypnoea; metabolic acidosis (lactate commonly high); hypokalaemia
This list is not exhaustive, see SPC www.hpra.ie for full details.
Ventolin® Evohaler 100microgram/puff
Salamol® Steri-neb 2.5mg/2.5mL
Ventolin® Concentrate for Infusion 1mg/mL