Prescribing and Administration Monographs
General Information
Clinical Guidelines and Protocols
Antimicrobial Guidelines
Disclaimer
Opioid Withdrawal, Sedation, Adjunct for Pain
Dosage: Starting dose 0.5-1microgram/kg PO/IV 6-8hourly. Dose may be gradually increased to 3micrograms/kg 6hourly.
Sedation in PICU
Oral: 1-2micrograms/kg 6-8 hourly. Increase if necessary to a maximum dose of 5microgram/kg.
Slow IV Bolus: Starting dose 0.5-1micrograms/kg IV 6-8hourly, increased as necessary to 3micrograms/kg IV 6-8hourly. Doses up to 5micrograms/kg 6hourly have been used.
Note: Intermittent dosing may be sub-optimal in achieving adequate levels of sedation - a continuous infusion should be considered.
Continuous Infusion: Loading dose of 1microgram/kg IV, followed by continuous infusion of 0-1microgram/kg/hour
Monitoring: must use apnoea and oxygen saturation monitor for first 48hours, especially if used in conjunction with opioids. BP/HR should be monitored where high doses (≥ 2micrograms/kg) are being used.
Opioid Withdrawal, Sedation, Adjunct for Pain
Oral: Starting dose 1-2micrograms/kg PO 6-8hourly. Dose may be gradually increased to 5 micrograms/kg 6hourly (Single dose not to exceed 300micrograms).
Slow IV Bolus: Starting dose 0.5-1micrograms/kg IV 6-8hourly. Increase if necessary to max dose of 5microgram/kg 6hourly (Single dose not to exceed 150microgram).
Sedation in PICU
Oral: 2-5micrograms/kg 6-8hourly PO (Single dose not to exceed 300micrograms)
Slow IV Bolus: Starting dose 1-2micrograms/kg IV 6-8hourly. Increase if necessary to max dose of 5micrograms/kg. (Single dose not to exceed 150micrograms).
Note: Intermittent dosing may be sub-optimal in achieving adequate levels of sedation - a continuous infusion should be considered.
Continuous Infusion: Loading dose of 2-3micrograms/kg, followed by continuous infusion of 0-2micrograms/kg/hour. Doses of up to 3micrograms/kg/hour have been used.
Pre-operative sedation – on the direction of a consultant only:
4micrograms/kg (maximum dose 300micrograms) PO as a single dose.
The onset of action of clonidine is at least 45-60 minutes. Administration of clonidine should be timed accordingly.
Baseline blood pressure and heart rate should be recorded prior to administration and monitored thereafter.
Palliative care: see APPM formulary for dosing in pain/sedation/spasticity in palliative care.
Weaning: Clonidine should be gradually withdrawn – abrupt withdrawal can result in rebound hypertension. Restlessness, palpitations, tremor, headache and abdominal symptoms have also been reported.
Suggested weaning regimen:
If patient is on clonidine and opioids/benzodiazepines for >2 weeks wean opioids/benzodiazepines first then wean clonidine.
Wean clonidine dose not the frequency. Monitor for rebound hypertension and withdrawal and adjust weaning plan if necessary.
Second line treatment for ADHD, Tourette’s Syndrome, adjunct to methylphenidate if sedation is a problem:
Initial dose 25micrograms PO nocte; increase by 25 micrograms PO nocte every two weeks. Maximum of 5micrograms/kg per day or 300micrograms/day, whichever is lower. Titrate dose against symptoms and blood pressure.
Dose may be given in divided doses if sedation is a problem. Monitor BP and pulse after starting treatment and after each dose increase
Use of medication in child psychiatry must be part of a multi-modal treatment plan and therefore should be reviewed regularly by a child psychiatrist who will advise on lower age limit, dose escalation etc.
Clonidine should be gradually withdrawn –abrupt withdrawal can result in rebound hypertension.
Neonates: must use apnoea and oxygen saturation monitor for first 48hours, especially if used in conjunction with opioids. BP/HR should be monitored where high doses (≥ 2micrograms/kg) are being used.
≥1 month: Always consider the patient's susceptibility to respiratory depression especially if used in conjunction with opioids. Consider apnoea and oxygen saturation monitoring. Monitor BP, HR on initiating treatment, after each dosage increase and where high doses are being used (≥ 3microgram/kg)
Oral:
Intravenous: Catapres® Injection 150microgram/mL
Compatible infusion fluids: Sodium Chloride 0.9% w/v or Glucose 5% w/v
Method of Administration:
Slow IV bolus over 10 - 15 minutes
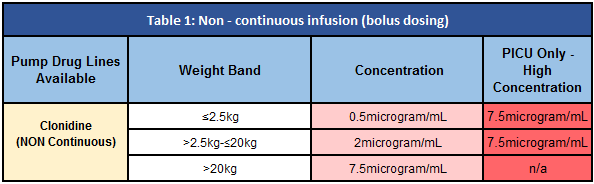
To accommodate measurement of smaller doses a ten-fold dilution is first recommended:
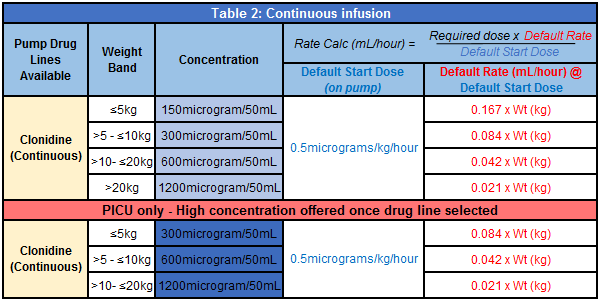
Continuous Infusion via the CHI Smart-pump Standard Concentration Infusion (SCI) drug library (Table 2).
Preferably administer via a central venous access device to avoid potential venous irritation as the preparation has a low pH.
Clonidine may potentiate the action of other CNS depressants such as opioid analgesics. Concomitant administration of opioid analgesics with clonidine also may potentiate the hypotensive effects of clonidine
When administered with other hypotensive agents, including diuretics, the hypotensive effect of clonidine may be increased.
Because clonidine may produce bradycardia and atrioventricular (AV) block, the possibility of additive effects should be considered if it is given concomitantly with other drugs that affect sinus node function or AV nodal conduction, β-adrenergic blocking agents (e.g., propranolol), calcium-channel blocking agents, or cardiac glycosides.
This list is not exhaustive. For full details see SPC www.hpra.ie
CNS: Inital sedation, headache diziness. Very rarely nightmares, perceptual disturbances
GIT: Dry mouth initially, nausea, vomiting and rarely constipation
CVS: Orthostatic hypotension (more likely at the start of treatment), bradycardia,
Skin: rash, urticaria may rarely occur.
This list is not exhaustive. For full details see SPC www.hpra.ie
Catapres® Injection 150microgram/mL
Catapres® Tablets 100microgram (may be crushed and dispersed in water)
Clonidine Tablets 25microgram
Clondine Oral Suspension 5microgram/mL (unlicensed)
Clonidine, when used as an adjunct to postoperative analgesic, should be weaned off before discharge from hospital.
Clonidine Oral Suspension is not routinely available from community pharmacies – if a child must be discharged on Clonidine Oral Suspension please contact the hospital Pharmacy department before discharging patient.
Opioid Withdrawal, Sedation, Adjunct for Pain
Dosage: Starting dose 0.5-1microgram/kg PO/IV 6-8hourly. Dose may be gradually increased to 3micrograms/kg 6hourly.
Sedation in PICU
Oral: 1-2micrograms/kg 6-8 hourly. Increase if necessary to a maximum dose of 5microgram/kg.
Slow IV Bolus: Starting dose 0.5-1micrograms/kg IV 6-8hourly, increased as necessary to 3micrograms/kg IV 6-8hourly. Doses up to 5micrograms/kg 6hourly have been used.
Note: Intermittent dosing may be sub-optimal in achieving adequate levels of sedation - a continuous infusion should be considered.
Continuous Infusion: Loading dose of 1microgram/kg IV, followed by continuous infusion of 0-1microgram/kg/hour
Monitoring: must use apnoea and oxygen saturation monitor for first 48hours, especially if used in conjunction with opioids. BP/HR should be monitored where high doses (≥ 2micrograms/kg) are being used.
Opioid Withdrawal, Sedation, Adjunct for Pain
Oral: Starting dose 1-2micrograms/kg PO 6-8hourly. Dose may be gradually increased to 5 micrograms/kg 6hourly (Single dose not to exceed 300micrograms).
Slow IV Bolus: Starting dose 0.5-1micrograms/kg IV 6-8hourly. Increase if necessary to max dose of 5microgram/kg 6hourly (Single dose not to exceed 150microgram).
Sedation in PICU
Oral: 2-5micrograms/kg 6-8hourly PO (Single dose not to exceed 300micrograms)
Slow IV Bolus: Starting dose 1-2micrograms/kg IV 6-8hourly. Increase if necessary to max dose of 5micrograms/kg. (Single dose not to exceed 150micrograms).
Note: Intermittent dosing may be sub-optimal in achieving adequate levels of sedation - a continuous infusion should be considered.
Continuous Infusion: Loading dose of 2-3micrograms/kg, followed by continuous infusion of 0-2micrograms/kg/hour. Doses of up to 3micrograms/kg/hour have been used.
Pre-operative sedation – on the direction of a consultant only:
4micrograms/kg (maximum dose 300micrograms) PO as a single dose.
The onset of action of clonidine is at least 45-60 minutes. Administration of clonidine should be timed accordingly.
Baseline blood pressure and heart rate should be recorded prior to administration and monitored thereafter.
Palliative care: see APPM formulary for dosing in pain/sedation/spasticity in palliative care.
Weaning: Clonidine should be gradually withdrawn – abrupt withdrawal can result in rebound hypertension. Restlessness, palpitations, tremor, headache and abdominal symptoms have also been reported.
Suggested weaning regimen:
If patient is on clonidine and opioids/benzodiazepines for >2 weeks wean opioids/benzodiazepines first then wean clonidine.
Wean clonidine dose not the frequency. Monitor for rebound hypertension and withdrawal and adjust weaning plan if necessary.
Second line treatment for ADHD, Tourette’s Syndrome, adjunct to methylphenidate if sedation is a problem:
Initial dose 25micrograms PO nocte; increase by 25 micrograms PO nocte every two weeks. Maximum of 5micrograms/kg per day or 300micrograms/day, whichever is lower. Titrate dose against symptoms and blood pressure.
Dose may be given in divided doses if sedation is a problem. Monitor BP and pulse after starting treatment and after each dose increase
Use of medication in child psychiatry must be part of a multi-modal treatment plan and therefore should be reviewed regularly by a child psychiatrist who will advise on lower age limit, dose escalation etc.
Clonidine should be gradually withdrawn –abrupt withdrawal can result in rebound hypertension.
Neonates: must use apnoea and oxygen saturation monitor for first 48hours, especially if used in conjunction with opioids. BP/HR should be monitored where high doses (≥ 2micrograms/kg) are being used.
≥1 month: Always consider the patient's susceptibility to respiratory depression especially if used in conjunction with opioids. Consider apnoea and oxygen saturation monitoring. Monitor BP, HR on initiating treatment, after each dosage increase and where high doses are being used (≥ 3microgram/kg)
Oral:
Intravenous: Catapres® Injection 150microgram/mL
Compatible infusion fluids: Sodium Chloride 0.9% w/v or Glucose 5% w/v
Method of Administration:
Slow IV bolus over 10 - 15 minutes
To accommodate measurement of smaller doses a ten-fold dilution is first recommended:
Continuous Infusion via the CHI Smart-pump Standard Concentration Infusion (SCI) drug library (Table 2).
Preferably administer via a central venous access device to avoid potential venous irritation as the preparation has a low pH.
Clonidine may potentiate the action of other CNS depressants such as opioid analgesics. Concomitant administration of opioid analgesics with clonidine also may potentiate the hypotensive effects of clonidine
When administered with other hypotensive agents, including diuretics, the hypotensive effect of clonidine may be increased.
Because clonidine may produce bradycardia and atrioventricular (AV) block, the possibility of additive effects should be considered if it is given concomitantly with other drugs that affect sinus node function or AV nodal conduction, β-adrenergic blocking agents (e.g., propranolol), calcium-channel blocking agents, or cardiac glycosides.
This list is not exhaustive. For full details see SPC www.hpra.ie
CNS: Inital sedation, headache diziness. Very rarely nightmares, perceptual disturbances
GIT: Dry mouth initially, nausea, vomiting and rarely constipation
CVS: Orthostatic hypotension (more likely at the start of treatment), bradycardia,
Skin: rash, urticaria may rarely occur.
This list is not exhaustive. For full details see SPC www.hpra.ie
Catapres® Injection 150microgram/mL
Catapres® Tablets 100microgram (may be crushed and dispersed in water)
Clonidine Tablets 25microgram
Clondine Oral Suspension 5microgram/mL (unlicensed)
Clonidine, when used as an adjunct to postoperative analgesic, should be weaned off before discharge from hospital.
Clonidine Oral Suspension is not routinely available from community pharmacies – if a child must be discharged on Clonidine Oral Suspension please contact the hospital Pharmacy department before discharging patient.